
He completely decimates them, see his breakdown here:

 vinayprasadmdmph.substack.com
vinayprasadmdmph.substack.com
Excerpt:
"Masking is a divisive issue, however, at the end of the day, it is a scientific question. Pre-pandemic, community masking was discouraged because the pre-existing evidence was negative. This is why Fauci was critical of it in early March 2020 on 60 minutes. In the pandemic, masking has become a marker of politics. Good liberals wear them and bad conservatives don’t.
As a scientist stuck in the middle, with my colleagues J. Darrow and I. Liu, we performed an umbrella review of this topic. We found very poor quality data, insufficient to support community masking, particularly for years on end. Cloth masks had especially bad data. Data to support masking kids was absolutely absent. Worse however, was how little we learned during COVID19.
The CDC did not run a single randomized controlled trial (RCT). An individual RCT called DANMASK was negative, but this trial was powered for a 50% reduction in infection. Some thought that was asking too much (we will return to this)! A cluster RCT in Bangladesh was negative for cloth masks, and very modestly positive for surgical masks. However, further data revealed imbalances in the starting size— likely because the trial failed to achieve concealment, leading more people to sign up in the intervention arm (who may be less committed to report + Covid symptoms; biasing results). Furthermore, absolute event differences were v small. These facts, combined with prior literature, suggest that confidence even in surgical masks is extremely low. Meanwhile, there are no RCTs in kids, a catastrophic research failure.
Enter a new study in MMWR— the CDC’s pet journal; It is getting widely tweeted and cited, and that is unfortunate. The paper is entirely, irredeemably flawed. Its flaws are so evident that it should not have been published nor promoted. When an issue is deeply polarizing, publishing bad science helps no one. It cannot convince skeptics, proponents don’t need convincing, and it deepens mistrust in institutions. Let’s consider the paper.

The paper is a case control, test negative study. Basically, anyone in California btw Feb and Dec 2021 who got a COVID19 test could be enrolled. People were told if they tested + or -. Two days later, someone tried to call COVID-positive people. 13.4% of people who tested positive answered the phone. For each positive person, a negative person matched by age and sex who was called was identified. Only 8.9% of people who tested negative answered the phone.
We could stop right now. Very few people answered the phone. Moreover, there may be a big difference in who answered the phone. A person sick enough to be tested for COVID, who was +, might not be doing so well 2 days later. Which ones answered? How about those who tested negative? Are thee comparable people? Sadly, researchers continued…."
================================================================================
Steve Kirsch does a great job summarizing Prof. Prasad's article:

 stevekirsch.substack.com
stevekirsch.substack.com
"I don’t care how you feel about masks, but this article is important. It shows you how totally inept and corrupt mainstream academia is.
In short, the CDC wants you to believe this chart is true:

But hang on a second. The same CDC nearly a year earlier told us that masks only reduce cases by less than 2%. So it’s super confusing, isn’t it? What changed? Which one should we believe?
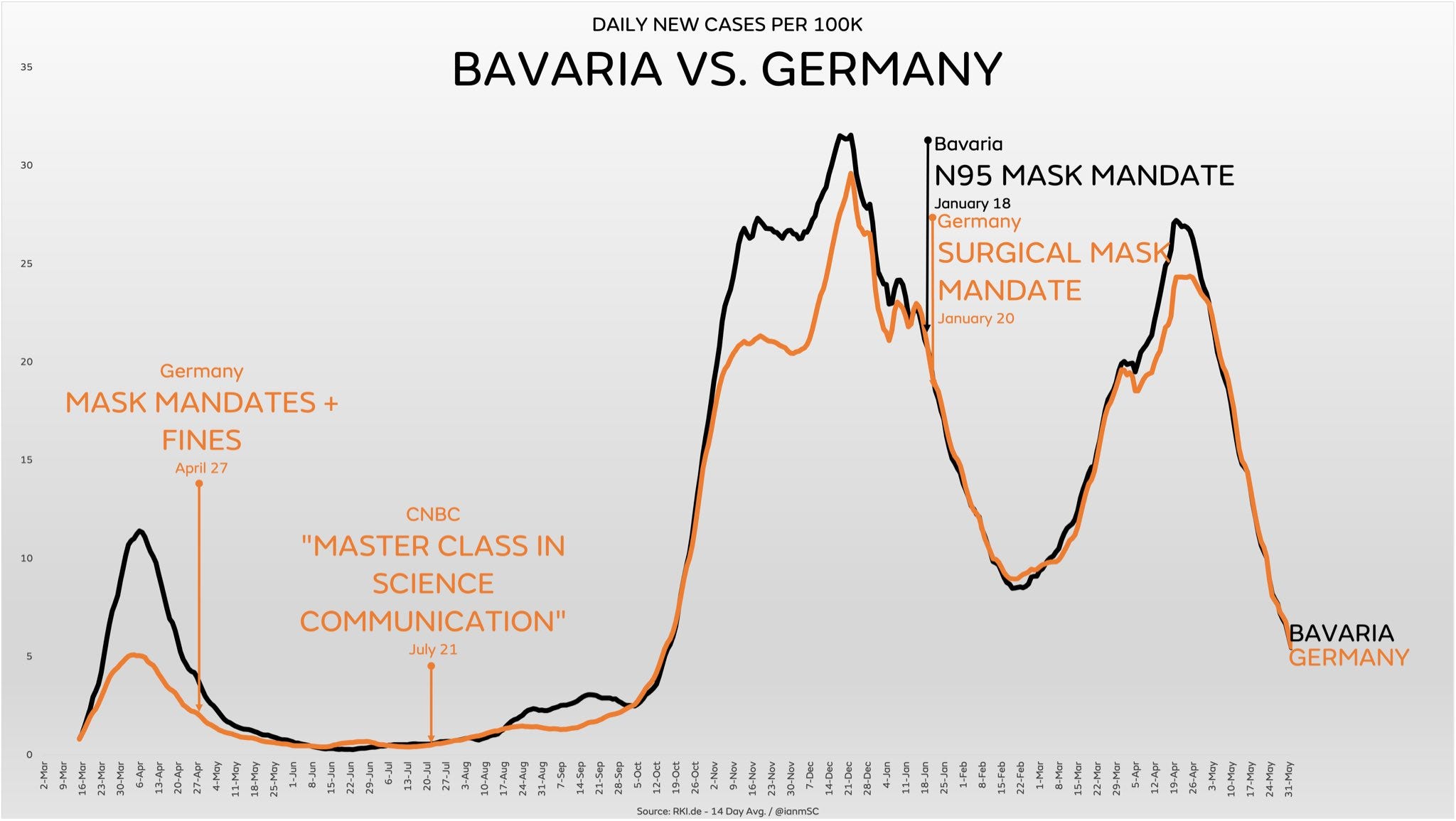
The truth is they are all zero and indistinguishable from doing nothing. Look at the real world results of mask mandates: the N95 area performs worse than the surgical mask areas.

And according to the WHO in 2004, surgical masks cannot stop a virus. In the WHO 2004 “Laboratory Biosafety Manual” (Third Edition) it says, “Surgical type masks are designed solely for patient protection and do not provide respiratory protection to workers.”
And of course both randomized mask studies showed no effect (if you actually look at the data). See the Masks section of Incriminating Evidence for all the detailed references...."
Mask studies reach a new scientific low point
MMWR appears to no longer be in the science business
vinayprasadmdmph.substack.com
Excerpt:
"Masking is a divisive issue, however, at the end of the day, it is a scientific question. Pre-pandemic, community masking was discouraged because the pre-existing evidence was negative. This is why Fauci was critical of it in early March 2020 on 60 minutes. In the pandemic, masking has become a marker of politics. Good liberals wear them and bad conservatives don’t.
As a scientist stuck in the middle, with my colleagues J. Darrow and I. Liu, we performed an umbrella review of this topic. We found very poor quality data, insufficient to support community masking, particularly for years on end. Cloth masks had especially bad data. Data to support masking kids was absolutely absent. Worse however, was how little we learned during COVID19.
The CDC did not run a single randomized controlled trial (RCT). An individual RCT called DANMASK was negative, but this trial was powered for a 50% reduction in infection. Some thought that was asking too much (we will return to this)! A cluster RCT in Bangladesh was negative for cloth masks, and very modestly positive for surgical masks. However, further data revealed imbalances in the starting size— likely because the trial failed to achieve concealment, leading more people to sign up in the intervention arm (who may be less committed to report + Covid symptoms; biasing results). Furthermore, absolute event differences were v small. These facts, combined with prior literature, suggest that confidence even in surgical masks is extremely low. Meanwhile, there are no RCTs in kids, a catastrophic research failure.
Enter a new study in MMWR— the CDC’s pet journal; It is getting widely tweeted and cited, and that is unfortunate. The paper is entirely, irredeemably flawed. Its flaws are so evident that it should not have been published nor promoted. When an issue is deeply polarizing, publishing bad science helps no one. It cannot convince skeptics, proponents don’t need convincing, and it deepens mistrust in institutions. Let’s consider the paper.

The paper is a case control, test negative study. Basically, anyone in California btw Feb and Dec 2021 who got a COVID19 test could be enrolled. People were told if they tested + or -. Two days later, someone tried to call COVID-positive people. 13.4% of people who tested positive answered the phone. For each positive person, a negative person matched by age and sex who was called was identified. Only 8.9% of people who tested negative answered the phone.
We could stop right now. Very few people answered the phone. Moreover, there may be a big difference in who answered the phone. A person sick enough to be tested for COVID, who was +, might not be doing so well 2 days later. Which ones answered? How about those who tested negative? Are thee comparable people? Sadly, researchers continued…."
================================================================================
Steve Kirsch does a great job summarizing Prof. Prasad's article:
Vinay Prasad exposes flawed CDC mask study and more ...
Updates on the deeply flawed CDC mask study, the Grand Jury starts, the J&J vax and Germany, and Santa Clara County, CA mandates
stevekirsch.substack.com
"I don’t care how you feel about masks, but this article is important. It shows you how totally inept and corrupt mainstream academia is.
If you were waiting for clear and convincing evidence that the mainstream medical community is totally brainwashed, this study is Exhibit A.
Take a look at this Twitter search result and you’ll see all the mindless regurgitation of the study without any critical thinking at all. Vinay is the only guy with a working brain.Nobody but Vinay Prasad would dare to call out the CDC on this. Vinay gets an A+ for having the courage to point out the obvious: that the Emperor has no clothes. Everyone else gets a fail: they eat it up without an ounce of critical thinking applied.
In short, the CDC wants you to believe this chart is true:

But hang on a second. The same CDC nearly a year earlier told us that masks only reduce cases by less than 2%. So it’s super confusing, isn’t it? What changed? Which one should we believe?
The truth is they are all zero and indistinguishable from doing nothing. Look at the real world results of mask mandates: the N95 area performs worse than the surgical mask areas.
And according to the WHO in 2004, surgical masks cannot stop a virus. In the WHO 2004 “Laboratory Biosafety Manual” (Third Edition) it says, “Surgical type masks are designed solely for patient protection and do not provide respiratory protection to workers.”
And of course both randomized mask studies showed no effect (if you actually look at the data). See the Masks section of Incriminating Evidence for all the detailed references...."
